About
You may need to undergo a surgical process if you have inflammatory bowel disease. You may wonder if there will be a change in the way you evacuate your stool after surgery. Generally, IBD results in the removal of the colon and/or rectum. The leftover active excretory tract has an end, which is usually where the small intestine ends. The surgeon pulls this end out through the abdominal wall to create a stoma. This entire diversion is known as an ileostomy. If the patient retains a segment of the colon as an active part of the excretory tract, the ostomy he gets is known as a colostomy.
With an ileostomy, also colostomy, you are going to have to wear an ostomy pouch over the stoma. This pouch collects bodily wastes.
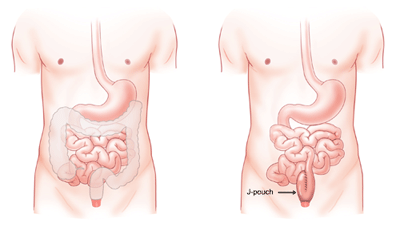
Another way to manage stool evacuation after the surgical removal of the entire colon is to have a J-pouch. This internal diversion, bypassing more precisely, allows the patient to evacuate bodily wastes through the anus.
Another way to manage stool evacuation after the surgical removal of the entire colon is to have a J-pouch. This internal diversion, bypassing more precisely, allows the patient to evacuate bodily wastes through the anus.
Ostomy surgery
IBD can result in either of two intestinal ostomies: ileostomy and colostomy. If the inflammation lies closer to the rectum and anus, the surgeon may want to cut the colon to separate the diseased part from the healthy part. Next, the surgeon pulls the end of the colon out through an incision in the abdomen to create an opening (stoma) for the waste materials to leave the body. This ostomy is known as a colostomy.
During ileostomy surgery, the surgeon removes or rests the entire colon after separating it from the small intestine. He then pulls the small intestine through an incision in the abdominal wall to create a stoma.
To manage both types of ostomies, you are going to need an ostomy pouch. Both ostomies can be permanent or temporary.
IBD can result in either of two intestinal ostomies: ileostomy and colostomy. If the inflammation lies closer to the rectum and anus, the surgeon may want to cut the colon to separate the diseased part from the healthy part. Next, the surgeon pulls the end of the colon out through an incision in the abdomen to create an opening (stoma) for the waste materials to leave the body. This ostomy is known as a colostomy.
During ileostomy surgery, the surgeon removes or rests the entire colon after separating it from the small intestine. He then pulls the small intestine through an incision in the abdominal wall to create a stoma.
To manage both types of ostomies, you are going to need an ostomy pouch. Both ostomies can be permanent or temporary.
J-Pouch surgery
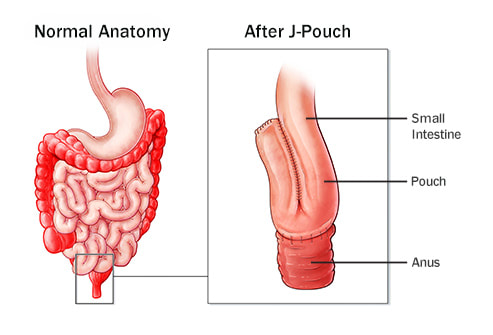
At the start, surgery involved in the creation of a j-pouch is pretty much the same as that of an ileostomy until the surgeon removes the colon. The additional part of this procedure, however, is the creation of a pouch of the end of the small intestine by folding it into itself. It forms the shape of ‘J’. The folding results in the formation of a reservoir that collects wastes. This reservoir is connected to the anus. When the reservoir fills with the stool, the patient feels the need to go to the toilet. The consistency of waste passing out of a j-pouch is the same as that from an ileostomy.
With a j-pouch, you may need to go to the toilet 3-6 times a day. It may decrease over time when your bowel adapts to its shortened length.
If you are to undergo surgery to remove the colon due to IBD, you may want to discuss with your doctor whether or not you can have a j-pouch.
With a j-pouch, you may need to go to the toilet 3-6 times a day. It may decrease over time when your bowel adapts to its shortened length.
If you are to undergo surgery to remove the colon due to IBD, you may want to discuss with your doctor whether or not you can have a j-pouch.
